For testing purposes, use the “Bogus Bank Online” (with an id and password) and the “Bogus Bank Over-the-Counter” payment channel simulators to test the behavior of online banking and OTC payments.
We feel free to contact them for assistance on the integration and they have helped us fully.
Following is the last form that we used to make before sending the data to the DragonPay
This Opencart 1.5.2.1 free module is with the price range filter module, it lists the range of prices and the products are filtered out as per the prices. Special thanks to me Rupak Nepali who work on Opencart module and provide most for free 🙂 After a long time, I worked in another opencart module Price range filter which refines Search as Per Price limits provided.
Download, documentation, and demo of the Price Range filter Module are below:
DOCUMENTATION You don’t need any programming knowledge to install this module. Just upload and enable the module, that’s all. If you don’t know how to upload the module then you can see this documentation. Install the Module After clicking the [Install] click [Edit] and set up the Price Filter module where ever you like to show.
Version supported: Opencart Version 1.5.6 tested but am sure it will support above 1.5.2.1
http://wordpress.org/plugins/file-away/ to show the sub-folders and show its files and folders respectively, though I am not able to work out in the plugin itself. This plugin displays file download links from your server directories or page attachments in stylized lists or sort-able data tables
Show files and folder in file away WordPress plugins
How I achieve it? I just worked in the plugin to show the directory and for the repetitive folder, I make another page and on another page, it shows up the list of the files and folders and shows it repetitively.
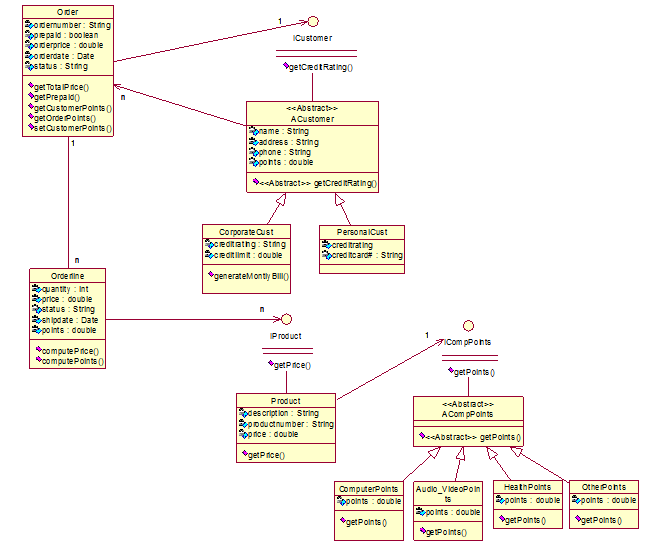
Question: Determine the classes needed for an order tracking system with the following specifications: Customers can place one order for any number of products. Every product has a product number, product description, and price. A customer can order more than one product at once (in one order). When a customer orders two products in one order, and product 1 is in stock and product 2 is not, then we ship first product 1, and later ship product 2. We need to keep track of the status of every order, and shipping date of every product. At this moment we make a distinction between corporate customers and personal customers. For all customers, we keep track of their credit rating. Corporate customers can have an excellent, good, or poor credit rating. Personal customers have by default a poor credit rating. If the credit rating is poor, then the order must be prepaid before we send out the product. This means that all orders from personal customers must be prepaid by credit card. If the credit rating is not poor, then the order does not need to be prepaid. Every corporate customer also has a certain credit limit. If the total order price is higher than the credit limit, the order must be prepaid. The system will generate a monthly bill for all corporate customers who did not prepay their order(s). When a customer buys a lot of products at our store, we want to reward that customer with a certain discount. If customers buy a computer-related product, then they get two points for every computer-related product they buy. For every health-related product, they get one point, and for every audio/video related product, they get 1/2 point. For all other products, they get 1/4 point. If customers accumulate 25 points, they get a 40% discount on their next order. If they receive this discount, then their number of points is reset to zero.
Although I have to determine only classes I have made the UML diagram so you can separate the classes as per your requirements:
Following are the classes that I have found appropriate:
Product
A Customer Corporate Customer Personal Customer
Order
Points
Computer Points
Audio Video Points
Health Points
Other Points
1. Product
The product should be in class because it is to be ordered by the customer and each product has some points.
2. Customer
A customer should be class because customers are the one who orders the products and they differentiate into two more customer corporate customer and personal customer.
Each corporate customer and the personal customer have their own characteristics so they must be made another class.
3. Order
Customer orders products so we need to take one class for each order.
4. Points
Each product has points assigned as per products. So there will be points class and its subclasses will be computer points, audio-video points, health points, and other points
Today we were working on the latest version of the jquery-2.1.0.min.js because our client sliced with the use of it. And we got the error because of the upper version and some method gets deprecated like Uncaught TypeError: Object [object Object] has no method ‘live’ as the live method is deprecated and removed from version 1.9 so need to change it to ‘on’. Thus we changed all .live into .on
We have also removed all the msie also $.browser.msie which was showing error like Uncaught TypeError: Cannot read property ‘msie’ of undefined
We have updated the catalog/view/theme/default/template/checkout/checkout.tpl and catalogviewjavascript/common.js
We need to update other files also product.tpl, register.tpl, cart.tpl, etc
Once you replace “.live” into “.on”, you will be able to remove the error.
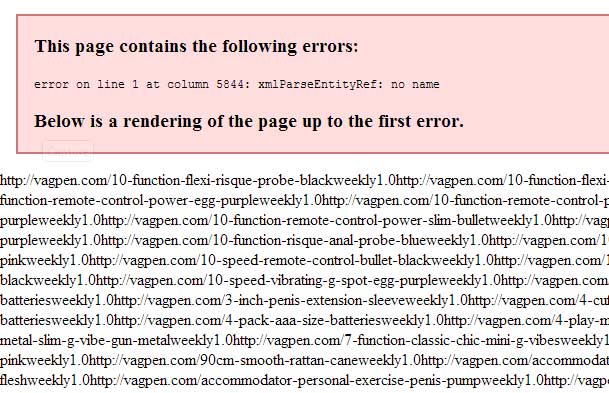
In Opencart we got the following error when we activated the Google Sitemap from Extensions>> Product Feed, then when we visited the google sitemap URL like Google Sitemap http://webocreation.com/index.php?route=feed/google_sitemap
This page contains the following errors: error on line 1 at column 5844: xmlParseEntityRef: no name Below is a rendering of the page up to the first error
xmlParseEntityRef: no name
How to remove it?
Go to PHPMyAdmin of the site and choose the database that you are using and in the oc_url_alias table, “oc_ is the prefix of the table”, search for the & and replace with something else like ‘-‘ or ‘_’ etc and the above error will be removed.
Let me know if you get something else and for support.
As opencart uses the SEO URL but we found most of the programmers are not using it in localhost, so today we are showing how to enable URL redirect in OpenCart in localhost. To use SEO URLs, the apache module mod-rewrite must be installed and you need to rename the htaccess.txt to .htaccess.
Enabling .htaccess in Xampp
Open the httpd.conf file with your favorite text editor. In XAMPP, this file is found in the apache/conf directory (or /LAMP/etc in Linux)
Locate the following line of code:
#LoadModule rewrite_module modules/mod_rewrite.so
Remove the # from the line as seen below to enable the module:
LoadModule rewrite_module modules/mod_rewrite.so
Save the Httpd.conf file
Restart your Apache Server
Now in the opencart admin activate SEO URL from
Admin>>System >> Setting >> Edit your store >>then at Server tab >> Enabled the SEO URL.
After that rename the .htaccess.txt to .htaccess
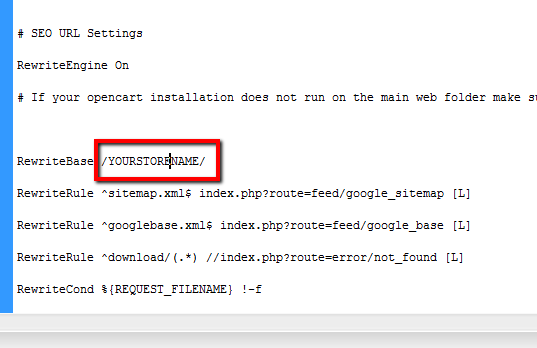
Now if your SEO URL does not work then find RewriteBase / / in .htaccess file and add folder name between slashes.
For eg: if your folder name inside the Htdocs is YOURSTORENAME then it will be
RewriteBase / YOURSTORENAME /
Make URL redirect in opencart at localhost
Then save and you will be able to work with the SEO URLs in localhost
We hope this opencart tutorial helps you understand the affiliate flow of Opencart 3. Let us know if you have any questions or suggestions, please subscribe to our YouTube Channel for Opencart video tutorials. You can also find us on Twitter and Facebook.
When we performed work at the scubattokki.com we have to remove Vqmod conflicts successfully for Opencart version 2. Some of the works we did are:
Remove the VqMOD conflict in opencart.
Checkout Steps decreased to two steps.
Registration pages change and address field changes
Korean Language translations
Many other small changes
How do we remove the VqMOD conflict?
They have used VqMOD like remove-add-to-cart-if-out-of-stock.xml, auto-reviews.xml, disable_affiliate.xml, ev_GridDefault.xml, featured-product-plus.xml, google_analytics_expert.xml, inmuto_hide_downloads.xml, inmuto_hide_wishlist.xml, remove-add-to-cart-if-out-of-stock.xml and many others like disabling captcha, etc
As they have used many VqMOD XML which changes the lines of codes and the remaining one does not find the code lines and occurs conflict likewise made the modifications on email format.
We checked what error is logged atVqMOD/logs and the files as per the day as we were working on Sunday so we checked at sun.log and find out what is the error and what search not found is logged. By this, we can know which XML is affected and we changed the code as per the requirement at a definite place to remove the conflict by this we were able to solve the conflict of VqMOD.
We have worked on the two-step quick checkout so that customers can easily check out by clicking only two clicks.
We have made many language changes as well as many CSS and registration page changes to hide the country, city, zone as he did not need them as all clients are from the locality.
About Scuba Bunny http://scubattokki.com/
Scuba Bunny http://scubattokki.com/
At Scuba Bunny http://scubattokki.com/, they search the world for the best quality scuba equipment at the best prices. Why are our prices so low? We import all our products directly from our suppliers in the USA and Italy. With no middleman, we pass the savings on to you! All items at Scuba Bunny are guaranteed to be brand new, original brand name products. All products come with original serial numbers and full warranty certificates.
Packt Publishing is launching an exciting campaign to coincide with the release of their 2000th title. During this offer, Packt is giving all its customers a chance to enjoy their books by giving them a free e-book copy for every purchase.
The campaign began on 18th March and will continue up until 26th Mar 2014.
You can find out who is using this offers by the social media hashtags #packt2k
Like for facebook, it is https://www.facebook.com/hashtag/packt2k, similar for the twitter and google plus.
If you want to excel in the OpenCart then you can get the following book
Today we completed two works to decrease the checkout steps where we have to combine the shipping and payment address at one as well as shipping and payment methods at another and transfer the shipping estimate to the shipping methods on the checkout step.
We made the shipping estimate on VqMOD and now the next work is to combine the checkout steps. Combine the shipping address and payment address at one step and shipping methods and payment methods on other steps.
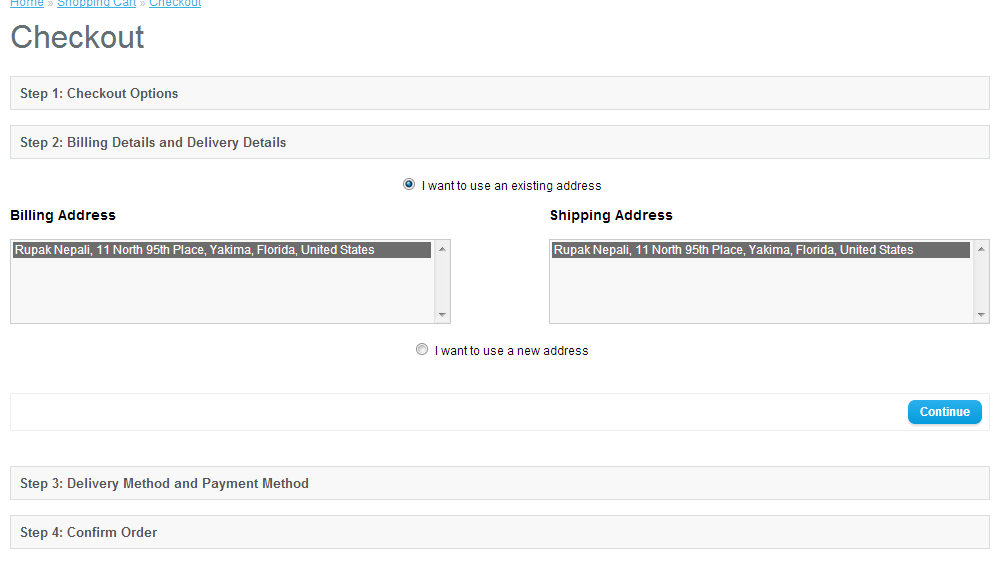
checkout_steps_decreased
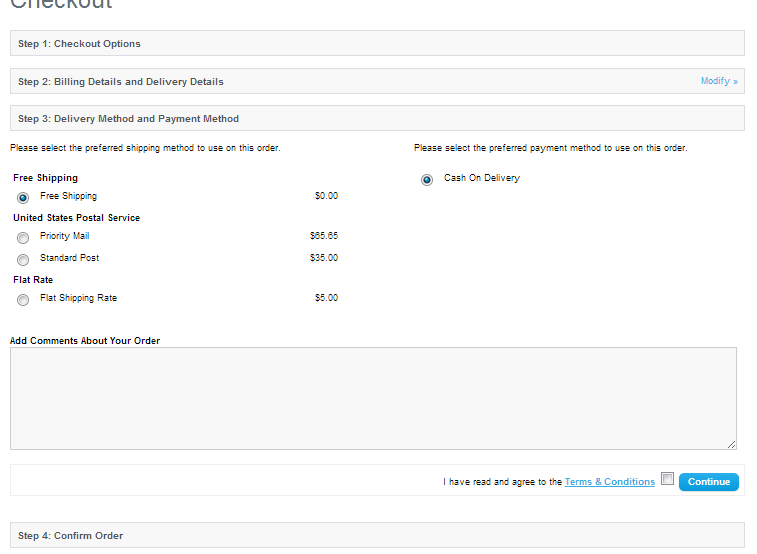
When the customer has logged in and checkout then it will show Step 2: Billing Details and Delivery Details, if the customer likes to change the address then he has to insert the new address and choose from the select list. After clicking continue it will redirect to Step 3: Delivery Method and Payment Method, where he has to choose the delivery method and the payment method. Then on clicking the continue, it will redirect to the confirmed section.
checkout_steps_payment_and_shipping
If the products don’t have the shipping then no shipping address and shipping methods are shown.
We are showing how to add Google Maps for opencart for free and show Google Maps on the contact us page and a module in the Opencart eCommerce website. This module works with VqMOD, if you like to manually insert the code read the post below which we will show how to do them.
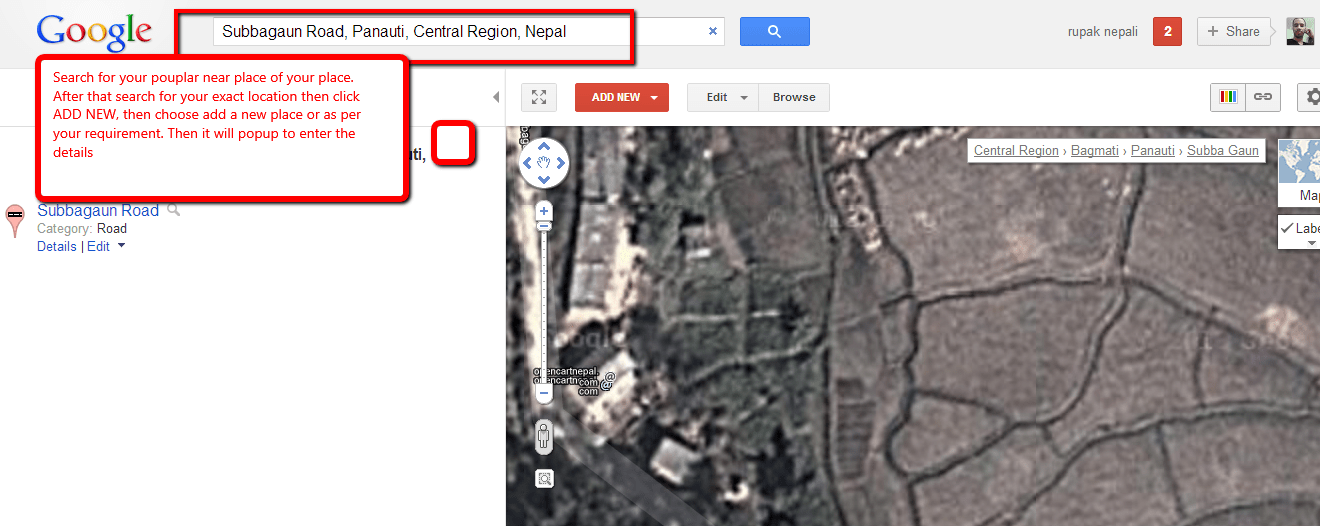
First, we like to show how to pin or add your shop locations on google maps. Go to http://www.google.com/mapmaker and search for the popular place near yours and zoom in to the map and see your exact location.
add your location to google map
Now click on the ADD NEW button and insert click to add the place and locate the red pin to your exact location and then insert the description as per required and SAVE. You can insert the phone, website, category, working hours, payment types, and so on.
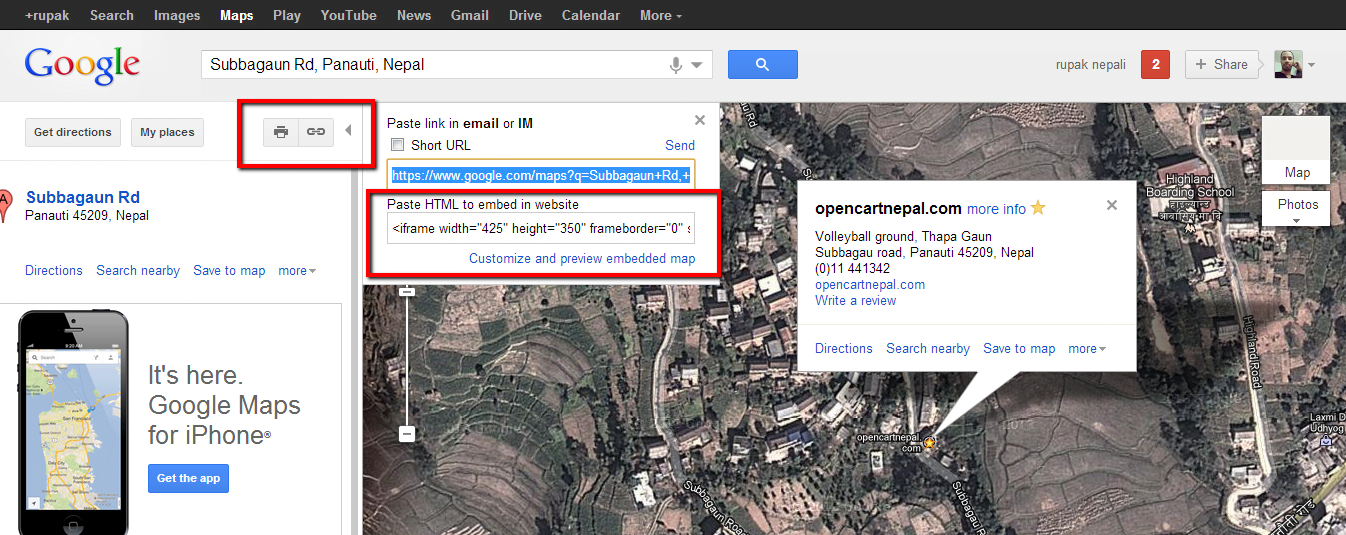
Now go to https://www.google.com/maps and search for your place and locate your place and pinned location. Google Maps will not instantly show your recently inserted location or shop. When you find your shop or location, then click on the red pin and it shows the details after that click on the link icon at the right (see the red box in the image below)
how to show the shop at the google map
Now find the HTML code and paste it into our contact google map module.
Now time to download the module and upload it to the respective directory.
1 Unzip in the folder. 2 Upload the files inside the googlemap folder to your OpenCart root folder. 3 In admin, go to Extension>> Module >>Google Map and install the module and edit.
Now time to insert the iframe HTML code that we get from the Google Map from above. Please edit the iframe width to 100% and height as per your requirement.
For mine code looks like below
<iframe width=”100%” height=”350″ frameborder=”0″ scrolling=”no” marginheight=”0″ marginwidth=”0″ src=”https://www.google.com/maps/ms?msa=0&msid=215707624648835363542.0004d48fa8b68dbc004b0&ie=UTF8&ll=27.597546,85.521119&spn=0,0&t=h&iwloc=0004d48fa8bb305cc3dfb&output=embed”></iframe><br /><small>View <a href=”https://www.google.com/maps/ms?msa=0&msid=215707624648835363542.0004d48fa8b68dbc004b0&ie=UTF8&ll=27.597546,85.521119&spn=0,0&t=h&iwloc=0004d48fa8bb305cc3dfb&source=embed” style=”color:#0000FF;text-align:left”>opencartnepal.com</a> in a larger map</small>
Then add the module to where you like to show in the layout. One of the interesting things of this module is that it will show google map  in the contact us page just below the details of the contact.
Vqmod is needed to show the google map at the contact us page. If you don’t like to show it at the contact us page then you have to delete the googlemap.xml at the VqMOD and install the module pack. If you don’t have the v=VqMOD and like to show the google map at the contact us page then you can easily use the module set to show at the contact layout.
COPYRIGHT:
This module code is the intellectual property of mine as an Opensource code you are entitled to use it freely and modify it if you wish but please keep the credits intact.
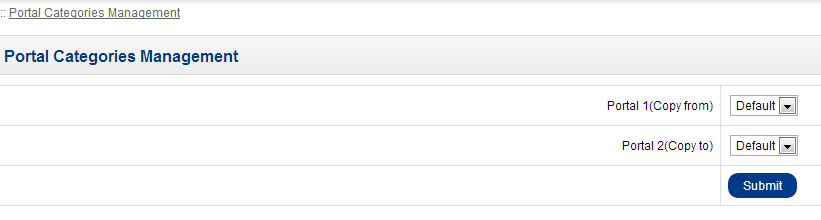
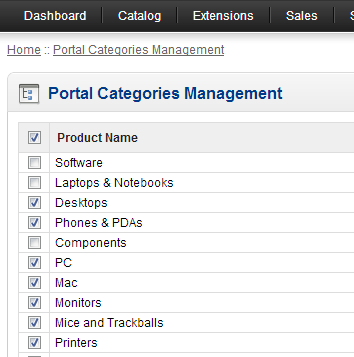
Bulk transfer of products, categories, and manufacturers to stores on Opencart eCommerce store
If you have already inserted the products and want to add the store in the Opencart eCommerce store, after this transferring the products to the store is quite tedious. You have to go to each product and check for the store and click save, to remove this tediousness, we have created the bulk transfer of products which helps in transferring the products between the stores of Opencart eCommerce.
1 Unzip in the folder. 2 Upload the files inside the bulk_transfer folder to your OpenCart root folder. 3 In admin, go to Catalog >> Bulk Category Transfer or Catalog >> Bulk Product Transfer or Catalog >> Bulk Manufacturer Transfer 4 vQmod is needed for the backend to see the Catalog >> Bulk Category Transfer etc
If you don’t have the vQmod installed then you have to insert the following lines at admin/view/template/common/header.tpl
Today we provide support to Opencart forum that someone appreciates my work as we have helped him with his e-commerce designs to show the first four menu items in Opencart.
We simply changed the code and posted it on the forum and his reply was:
You, my friend, are a legend! That is exactly what I was looking for. Thank you so much! its really appreciated. I just checked out your website, some useful information on there, bookmarked
University of West London
School of Computing and Technology
Student Assignment S1
Title
UML Component Modelling Assignment
Module
UML Component Modelling
Module Code
CP70008E
Module Leader:
DrNasser Matoorian
Set by:
DrNasser Matoorian
Moderated by:
Dr Samia Oussena
Assignment
Assignment
Hand in arrangements
The modelling element 3 of this assignment must be submitted via Blackboard.
Structure of assignment
This assignment has three elements. The learning outcomes of the module are assessed by a successful completion of the elements.
Element
Type
Weighting
Due Date
1
In-class Viva and Presentation (Business Process Model)
5
Week 8 – Nov 21, 2012
2
In-class Viva and Presentation (Use Case Models and Business Concepts)
15
Week 11 – December 12, 2012
3
Component Model
80
Week 14 – Friday Jan 18, 2013
Extensions will only be granted in exceptional circumstances. Extensions will be for 10 days or less. Documentary evidence will be required. Extensions must be agreed before the deadline. Submissions up to one week late with no extension will be marked with a maximum mark of 50%.
Learning outcomes
1
Analyse and design component based architecture solutions
2
Evaluate and articulate the rationale for alternate component implementation technologies.
3
Display mastery of knowledge in current and future software development practice using component based approaches
4
To understand modern approaches to component implementation technologies.
Element 1
Title
In-class Viva and Presentation (Business Process Model)
Task details
A case study accompanies this section of the assignment. It describes the requirement for a system within a business context. You will need to make assumptions in the course of constructing your models. Ensure you submit a list of these assumptions with your assessment elements as appropriate. If you are at all unsure about the case study description you should ask questions within the seminars/workshops. The Tutors will be moderating the discussion boards. The diagrams must be completed using a CASE tool (starUMLis a suitable tool).You need to present the BPM elements of your work to your tutor and be able to answer questions.
Marking Guide
Criteria
Issues
Mark
Marking breakdown where appropriate
Business Process Model
A Process Model with appropriate tasks.
5
Element 2
Title
In-class Viva and Presentation (Use Case Models and Business Concepts)
Task details
A case study accompanies this section of the assignment. It describes the requirement for a system within a business context. You will need to make assumptions in the course of constructing your models. Ensure you submit a list of these assumptions with your assessment elements as appropriate. If you are at all unsure about the case study description you should ask questions within the seminars/workshops. The Tutors will be moderating the discussion boards. The diagrams must be completed using a CASE tool (starUMLis a suitable tool).
You need to present the Use case diagram and the Business Concepts diagram of your work to your tutor and be able to answer questions.
Marking Guide
Criteria
Issues
Mark
Marking breakdown where appropriate
Â
Use Case ModelÂ
Â
Business Concepts
Â
Type Model
A Use Case diagram showing the system, the actors and the use cases for the system.
A class diagram showing all the key concepts in the case study and their relationships.
A class diagram showing Core Types and Business Components
5
5
5
Element 3
Title
Component Model
Task details
A case study accompanies this section of the assignment. It describes the requirement for a system within a business context. You will need to make assumptions in the course of constructing your models. Ensure you submit a list of these assumptions with your assessment elements as appropriate. If you are at all unsure about the case study description you should ask questions within the seminars/workshops. The Tutors will be moderating the discussion boards. The diagrams must be completed using a CASE tool (starUML is a suitable tool).
Marking Guide
Criteria
Issues
Mark
Marking breakdown where appropriate
Business Process Model
A Process Model for each key life-cycle in the application. Swim lanes Indentified with appropriate tasks.
10
Use Case Model
A Use Case diagram showing the system, the actors and the use cases for the system. Each Use Case should have a description including a scenario. Careful to show extensions and exceptions where appropriate.
20
Diagram and Explanation (10)
Use Case Descriptions (10)
Business Concepts
A class diagram showing all the key concepts in the case study and their relationships.
15
Type Model
A Type model class diagram showing appropriate core types and business component.
15
Component Specifications
Business rules (invariants), identification of business and system interfaces.
10
Business Rules (5)
System Interfaces (5)
Component Architecture
Component Diagram showing links between interfaces and a description of the communication between components via the interfaces.
10
Component Architecture (5)
Interaction Diagrams (5)
Grade descriptors
In addition to the assessment criteria above the following table may assist you in understanding how we arrive at your final mark. Indeed your final mark should agree with the following grade descriptors, but note that the assessment criteria are the main means of assessment.
Mark
Descriptor
0-39%
Limited conceptual understanding with possible structural deficiencies. Restricted use of theory within module. Inappropriate argument leading to unreliable and invalid conclusions/recommendations
40-49%
Some confusion in purpose & aims of evaluation. Some overall structure and conceptual understanding. Fair use of theory but arguments sometimes irrelevant, illogical or with unsupported assertions.
50-59%
Demonstrates a limited but accurate level of understanding presented in a mostly descriptive manner. The answer contains relevant interpretation and critical understanding especially at the upper end of the marking range.
60-69%
Demonstrates accurate knowledge and understanding of the subject presented in a coherent manner. The answer contains evidence of application and interpretation. At the upper end there is evidence of thoughtful and measured critical evaluation.
70-79%
Demonstrates a clear, comprehensively researched understanding of relevant material with some element of critical evaluation. Shows initiative in approach and rigour in the handling of information. Demonstrates originality of thought together with interpretation and application to the relevant sector
80% or above
The answer is analytical and critical. The assignment demonstrates scholarship through a depth of insight and understanding of relevant material, which is logically structured, accurate and well referenced. Originality of thought and application is evident.
Case Study
LH MedicalCompany (LHM)
LHM is a London based privately owned hospital which provides health care to its patients. The hospital uses in-house software to manage and service its patients which they refer to as clients. It is an expanding venture and needs to accommodate for processing its information globally. The practice management system is web-enabled and multi-platform for connectivity via web services, in addition, it has connectivity to existing legacy systems. An enterprise document management system ensures patient documents are replicated globally and available per demand.
In addition to medical treatments, medicine, and drugs, consultation and vaccinations are offered to its patients (with a variable additional fee) the company offers medical instruments to other companies either to purchase or to lease.
LHM records the details of its clients with possibly their full medical history in their computer system. When a new patient requests an appointment (walk-in or online) a treatment course begins and a practitioner is allocated to the patient. A full history and previous medical records are printed showing different categories of Treatments during different time intervals. Analyses are drawn in terms of any possible allergies and previous histories. Treatments may involve many surgeons and consultants depending on its complexity.
The contact practitioner is responsible for estimating the costs of treatments that is agreed by the client at the start of the treatment. The duration of the treatment may be set at any time duration and may also be changed during the treatment depending on the complexity of possible operations. The final cost and completion date are recorded at the end of the treatment.
During a treatment process, notifications may be sent to patients and other practitioners.
Repeat prescriptions may automatically be produced by the system if appropriate and are available for collection at any surgery by the patient. At any time a practitioner may suspend or cancel the prescriptions.
The cost for a treatment is paid for by the client or an insurance policy provided by a number of insurers. Insurance policies may have additional surcharges and cost depending on treatment types and medicines. Long-term treatment courses may be edited or canceled by practitioners or clients. To re-start an existing treatment an additional fee is applied.
LHM may receive requests for specialise treatments from other hospitals or they may refer clients to other medical centres.
Each treatment course or service may include one or more of the following items:
Operations and vaccinations
Consultations and check-up
Medicine and different types of tablets
Clinical reports and attached documents and history
Prescriptions and repeat Prescriptions
Payments by clients may be in full or part payments to cover a range of medical and non-medical services offered by the company. Payments may include possible applied surcharges for late payments and or special discounts for long-term treatments. Tax allocations may also vary from one treatment item to another. Payments have to accommodate for price changes for medicines and medical services and track price changes for drugs purchased from pharmaceutical companies.
A treatment course comprising services from other hospitals carry additional changes set by the medical service providers. A full list of Treatment courses with corresponding payments may be requested by the site manager at any time. Clients’ outstanding balances may be retrieved at any time for current treatment and services indicating the payments for the treatment course.
If you are an admin you can do the following steps:
1. Make one fake customer. 2. Set the site into Maintenance Mode, be sure you keep on logging to the admin 3. Now activate the Cash on the Delivery method of payment. 4. Complete the buying process with many quantities with the use of the Cash on the delivery payment method
In this way, we can show the products into the best sellers.
If you are looking to show or add the bestseller module in pages then this video will help you:
Today I am very amazed why the following templates are free. I was just searching for the free template found out a bunch of themes that are free and have a great standard.
In this college internship report, we are showing online earnings and website programming recommendations, conclusion, program workplace relationships, and bibliography.
CHAPTER FOUR
Recommendations
There are few things which can be implemented and improvements can be made.
There must be a career development opportunity for the employees so that they can work energetically in the organization as there is high turnover due to lack of information in the related sector.
The remuneration System must help in motivation as a better remuneration package can do more in this highly competitive environment.
The work environment at DP Sign is such that it does not encourage the staff to work effectively and I recommend that jobs should be such that the worker really enjoys what they are really doing.
The staff as an individual is good but as a team is very bad, this thing should be overcome by promoting the team-based culture by the company.
What I feel while working in DP Sign was that the top management is taking HRD as an expense rather than an investment as in the future the real capital or asset will be in the form of the workforce rather than monetary capital.
In DP Sign there are uses of advanced technology so the employee outside the world cannot cope easily with the internal environment so the socialization process should perform while recruiting the new employee.
I suggest DP Sign to make a website to unite their online earning team and the exchange of click can be done so that everyone can get benefits.
There are problems in web hosting services as the mail is sent to the scams sector so it should be maintained and the reliable up to date time is 98% only so the web hosting services should be changed.
CHAPTER FIVE
Conclusion
The internship program is one of the training that helps students to learn a lot and my vision and practical exposure have broadened very much from my three months internship.
In the website development and online earning sector, DP Sign is contributing a lot and is using modern technology to take the company to new horizons and is moving as per its slogan “A strategic partner of our clients, not a mere vendor”.
After doing my internship it becomes clear to me that books are only dealing with the ideal situation while in the real world it is not so, and you have to face many problems particularly in programming and designing field in which you are dealing with codes and the behavior of software to handle them. Besides this, I just came across with abstract and the concepts developed with thorough study able to make a vague mental image while working in a real scenario.
Further, I also concluded that 100 percent concentration, full care, analytic descriptive, knowledge and communication skills are the key prerequisites for working in the real world.
Anyhow, precisely speaking this internship of three months is a memorable period for me during which I availed the opportunity to flourish my communication skills, polish my capabilities and abilities, upgrade my knowledge about the latest technology and application tools and broaden my vision and exposure towards practical life.
This internship proves better for me in two way, on one side it helps to develop a personality in me which exactly match the professionalism in web development and secondly it helps to strengthen my decision about the specialization in web technology as my personality exactly match the nature of the job.
CHAPTER SIX
PROGRAM WORKPLACE RELATIONSHIP
This project has proved to be very useful in putting the theoretical knowledge learned in college into practical knowledge. Through this project, the various subjects learned by us such as the principle of management, system analysis, and design, C programming, web technologies, Object-oriented languages, organizational behavior, and other programming have been put into use practically.
The subject matter of system analysis and design and other programming languages and web technologies learned theoretically were put into use in this project. Planning of the assignment, locating information sources, collecting and analyzing data, presenting charts and tables, programming, website designing and programming, understanding system and software as well as re-engineering them, etc. which are already studied by us in books was very helpful in putting it into practical experiences and preparing this project. The theoretical knowledge of web technologies, programming languages and managerial courses were helpful in carrying out the SWOT analysis, PEST analysis, and other analysis.
This program is very helpful in putting our theoretical knowledge into practical knowledge. All the subject matter studied by us in the previous semester was put into use while carrying out this project. Studying books is a different thing and going through all the things studied is different. This program has provided a platform to undergo real-life problems and experiences of business which will be fruitful to us in the coming years
BIBLIOGRAPHY
Book References:
Annual Report of DP Sign
Operating Manuals of the DP Sign
Publications of the DP Sign
System Analysis and Design Methods, McGraw-Hill Companies
Internship Report Management Information System, Prentice Hall
Software Project Management by E.M. Bennaton Second Edition.
DP Sign has different strategic business units and management as DP Sign is well aware that how to use these units strategically. In order to fully analyze the business units of DP Sign that are web development, online earning training, and printing, I have used different analysis which not only gives the true picture of the company’s different unit but it also gives the depiction of the overall industry analysis in which the company is currently working. There are four types of Analysis which I have performed in order to explore the working of the organization.
3.1.1Web Development department Analysis
3.1.2 Online Earning department Analysis
3.1.3 PEST Analysis
3.1.4 SWOT Analysis
.
All these analyses have been performed by getting data from real-time industry situation as well as the organization. Research articles, news articles, internship reports, manuals are being used in order to effectively analyze the working of the organization. The historical data for the analysis has been taken or maximum 5-7 years back while current data till 2009 has been used.
3.1.1 Web Development department Analysis
Present status of Website development in DP Sign
Though the Website development in Nepal is developing and every year many companies are being registered but the professional person is lacking in our country. DP Sign is also facing the same problem so it is hiring professional from other countries. Like other company in Nepal, DP Sign is also lacking local customer as our country is lacking the knowledge to use technology and computers.
But the use of technology and website in Nepal is also increasing thus DP Sign also has to focus on the local customers. Even personal website are taking market so DP Sign should focus on this site by reducing the costs but increase the volume of sale which ultimately leads to an increase in the profit.
Schools, college, institutions, shopping center are increasing thus DP Sign should focus in this sector also. One of the lackings of the DP Sign is that it lacks advertisement.
DP Sign has to face competition from:
Strong local market
New entrants in the international market
Competition from existing customers
Economic recession
From the strong local market, the competition has been arising from a few companies. These companies are well renowned not only locally but also internationally. In these local companies, DP Sign has been facing competition at website development. At locally and internationally DP Sign is facing the competition as the number of companies is increasing. As the economic recession is a period of recession and throughout the globe world is suffering from the economic crisis, in such a scenario, there is an effect on website development also.
In the context of DP Sign, the market capture internationally is very low in the context of other website company so the company should focus on maintaining the international customers.
3.1.2 Online Earning department Analysis
In the context of D.P. Sign Online Earning training generate about 15% of the Revenue. So this is also one of the most important departments of DP Sign but DP Sign is not focusing on it.
Internet in Nepal is increasing. Some business and people are eager to earn online by sitting at home and being boss of themselves so the online earning has also potential market to earn.
But DP Sign is not focusing in this sector and I suggest them to make a website to unite their team and exchange of click can be done so that everyone can get benefits.
3.1.3 PEST Analysis
PEST analysis is the analysis which we tend to perform in order to analyze the external as well as the internal environment in which the organization is currently working. PEST analysis revolves around the four things.
Political Environment
Economic Environment
Social Environment
Technological Environment
Political Factors
There are many factors, which entice the organization with Government.
Tax policy
Quota
Cyber Laws
Online transactions law
Labor policy
Economic Environment
Recession, devaluation of currency and the policy of government have an adverse effect in the economy.
Social Factors
Due to the increase in education and technological sector, the educational power of the customers is increasing at a speedy rate. They are becoming aware of the brands and the latest technology. Due to this, they are demanding high technological website at a low price in the international market.
Technological Factors
Technology is also a key sector in term of the external environment for website development. The technology is working as a substitute for manpower with more efficiency. DP Sign has to focus on following
Error reduction
Less labor cost
DP Sign should have to focus on maintaining the harmony between the factors of PEST analysis so that it can progress in its life cycle.
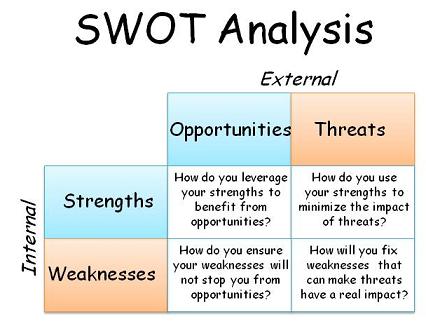
3.1.4 SWOT Analysis
Performing a SWOT analysis involves the generation and recording of the strengths, weaknesses, opportunities, and threats in relation to a particular task or objective.
Strengths
Strong and Prominent International Image
Latest Technology
Competitive Workforce
Creativity and Innovation
Management Information System
ISO Certified Company
Locally Working(Expenses in NRs but earning in Dollars)
Weaknesses
Individualism
Low Production capacity
No opportunity for Training and Development
Lack of teamwork
Lack of continuity of Policies
Too much Specialized Jobs
Opportunities
New Emerging Markets
Bright Local Market
New Cyber laws and Policies
Implementation of technology and websites in the government sector
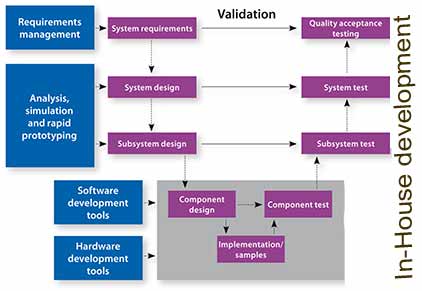
Website development in DP Sign is done in two ways, either it is built in-house or it is bought.
2.14.2.1 In-House Development
2.14.2.1.1 Design the application architecture
Application architecture defines the technologies to be used by one or more or all information systems in terms of their data, processes, interfaces and network components. In DP Sign database like MSQL, SQL, Oracle, MySQL etc were in use, I use MySQL. They use .net and PHP as the programming language and I prefer to use PHP language in website programming.
Physical data flow diagram is used to establish physical processes and location issues.
2.14.2.1.2 Design the database(s)
The purpose of this task is to prepare technical design specifications for a database that will be adaptable to future requirements and expansion. System analyst also participates in the database modeling and the system designers are responsible for the completion of the activity as databases are shared resource.
The database schema is also structured.
2.14.2.1.3 Design the system interface
In this, the system designer works with the system to develop input, output and dialogue specifications. For output, the terminal screen or the printed papers were used and for input, the data capture method is used.
System designers are responsible for the task and can use GUI (graphical user interface). For this, I have used Macromedia Dreamweaver and Phpmyadmin.
2.14.2.1.4 Package Design Specifications
The final design task involves packaging all the specifications from the previous design tasks into a set of specifications that will guide the computer programmer’s activities during the construction phase of the systems development methodology.
2.14.2.1.5 Update the Project Plan
Revaluation of the project is done. The project manager in conjunction with system owners and the entire team facilitates this task
2.14.2.2 Buy Solution
If the DP Sign is willing to buy the website from the outsider then following is done:
2.14.2.2.1 Identify and Research Specific Products
In this task, we research technical alternatives. The requirements specify the functionality, features and critical performance parameters for our new website. Research and information are collected from internal standards, information services, trade newspapers, and periodicals offer. System Designer with help of project manager is responsible to complete the task
2.14.2.2.2 Solicit Proposals or Quotes from Vendors
The solicitation task requires the preparation of RFQ (Request for Quotations) and RFP (Request for proposal). Request for Quotations is a formal document that communicates business, technical and support requirements for the application software package to a single vendor that has been determined as being able to supply that application package and services.
Request for proposal is also a formal document that communicates business, technical and support requirements for an application software package to vendors that may wish to compete for the sale of that application package and services,
2.14.2.2.3 Select and recommend the best vendor.
The purpose of this task is to validate requests for proposals and/or quotations received from vendors. Designer involves data and database administrators, network administrators and applications administrators. The key outputs of this task are those vendor proposals that proved to be validated proposals or claims and others whose claims were not validated.
2.14.2.2.4 Contract with the awarded vendor to obtain the product
Having ranked the vendor proposals the next activity usually includes presenting a recommendation to management for final approval. Salesmanship and communication skills are important. The purpose of this activity is to negotiate a contract with the vendor who supplied the winning proposal and to debrief the vendors that submitted losing proposals. A contract will be produced to the winning vendors.
2.14.2 Online Earning Department
2.14.2.1 Online Earning Training:
In this training, we were taught that how we can earn money online without investing money. This training last for 15 days for normal computer operator and for advance the time period is less. Online earning can be done by different means in this global market. Some of them are:
2.14.2.1.1 Online earning through blogging:
Blog or Weblog is nothing but the personal website where you can express your personal views, ideas, feelings etc. There are many sites such as Blogger, Typepad, Soulcast who provide blog services. You can earn online through Adsense. Here you have to place Adsense ads in your blog. You will earn whenever viewers click on the ads.
2.14.2.1.2 Online earning through Ad Typing:
Online earning by Ad typing is another unique job opportunity. All you have to need to post Ads on various Free Ad sites. There are tons of sites that provide Ad Typing jobs. Typeinternational is a very popular site. Typeinternational is providing nine different homes based earnings opportunities.
2.14.2.1.3 Online earning through Medical Transcription:
Medical Transcription is the fastest growing fields in health care. It is the process where you need accurately and swiftly transcribes medical records dictated by doctors and others, including medical history and physical reports, X-ray reports and pathology reports etc. Good English pronunciation, typing skill and acquaintance with medical terminology are the basic need of the job. You can earn lots of money through Medical Transcription.
2.14.2.1.4 Online earning through the filling of Market Survey Forms:
Filling of Market Survey Forms is another popular online job opportunity. Thousands of consumer products are fighting to get a pie of the billions of consumers worldwide. You can earn by simply filling up of forms regarding a particular product of a company.
DP Sign was founded in 2007. So it is a newly entered company in the corporate world. But its sale figures are outstanding. The company has sales of over 10 million Nepali rupees in the financial year 2008-2009.
The overall sales volume is generated from three areas domestic, commercial and International. The prices of the products of the company range from Rs. 350(Domestic) to Rs. 1.5 million.
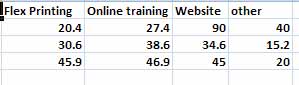
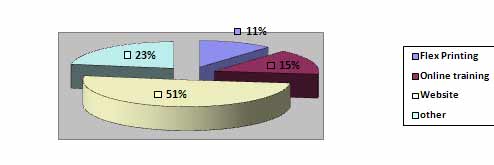
The Major portion of the revenue of DP Sign is Flex Printing, Online earning training, and website designing and programming.
The partition of sales to total sales graph is given below:
Fig: 2.2 Business volume of DP Sign
According to the figures company’s 51% sales of Revenue is earned through website designing and programming, 11% of revenue is from flex printing, and 15% and 22% are from online training and other sources respectively
Although DP Sign was founded in 2007 bt remained successful in getting its share in the market in a very short time (2007-2009) and through its loyal, devoted, professional and hardworking management it is expected that the company will expand its sales to about 4 million during 2010-2011.
Beside that company has also earn an impressive goodwill in the market through its quality services.
2.17 Products offered by DP Sign
2.17.1 Printing Services
SN
Material Type
Rate
Remarks
1
Printed backlit with box & light with fitting at site
199.00p.sq.ft.
Without vat
2
Vinyl sticker cutting & pasting on backlit with box & light with fitting at site
Search Engine Optimization(twitter marketing, social marketing, facebook marketing, affliation program)
As per design and requirement
7.
Online Earning Training
Rs 1500+
Tab: 2.7 Web services providing by DP Sign
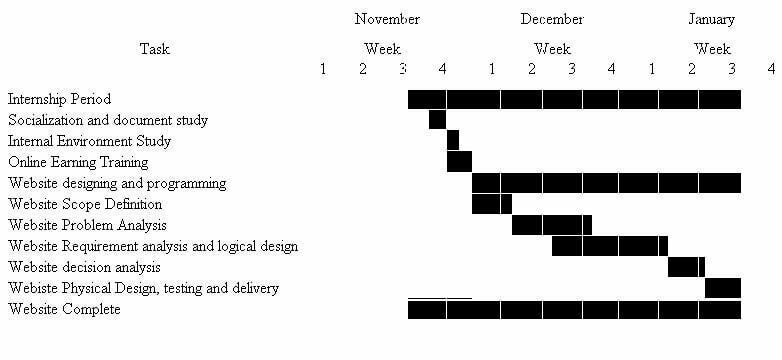
2.18 Time Frame of Internship
Fig: 2.3 Time frame representation in Gantt chart
The Gantt chart above depicts internship task against a calendar where each bar represents a named project task and the task are listed in the left-hand column.
Time frame representation in Gantt chart internship report